
Latest News
Is Kaiser’s Labor-Management Model Unraveling?
Health care workers say the system’s push for growth is undermining a once-vaunted partnership — and affecting patients.
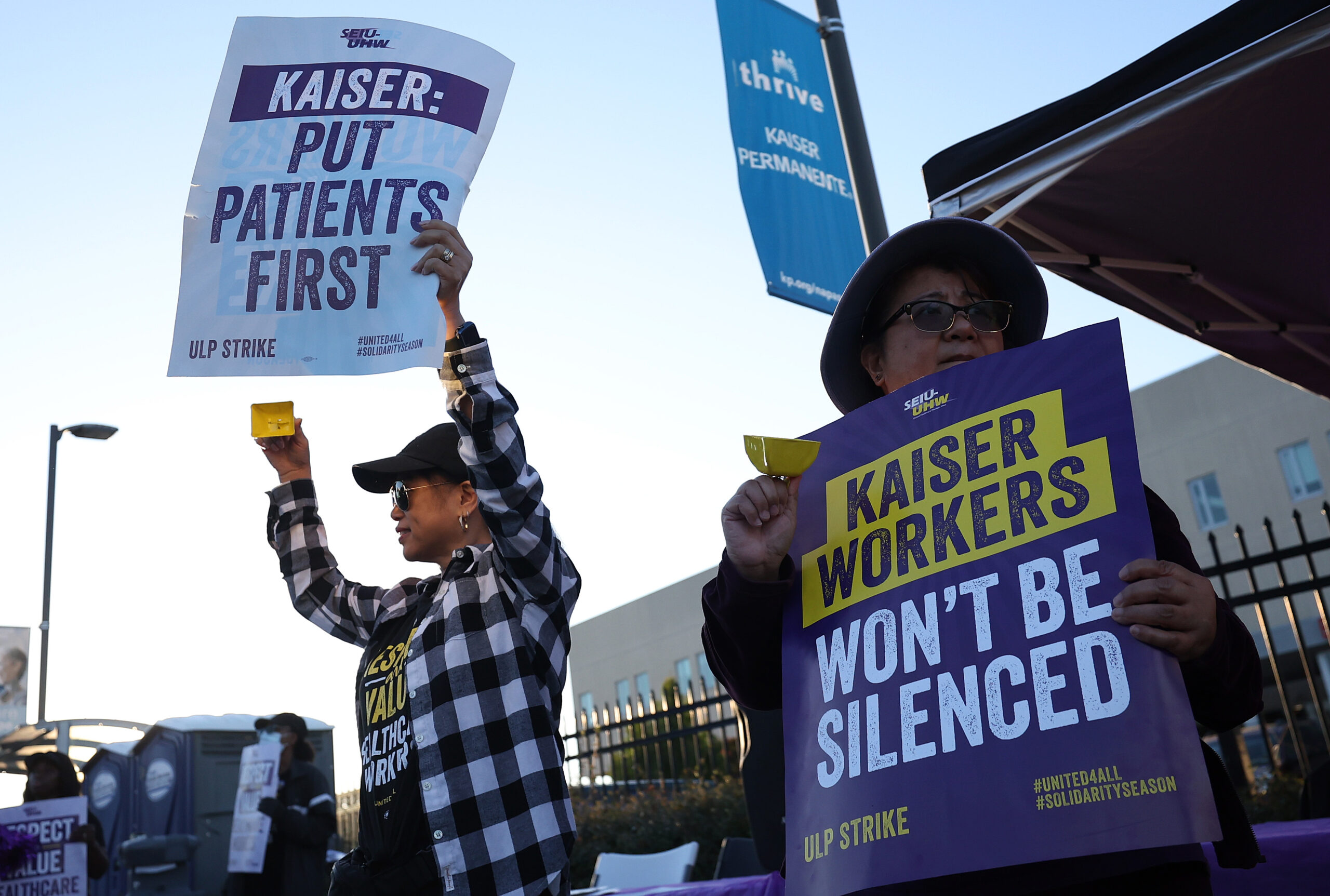
As California-based health care giant Kaiser Permanente has fought one battle after another with its unionized workers in recent years, what began as a murmured question is becoming a shout: Has the organization’s vaunted Labor-Management Partnership run its course?
The answer affects the 150,000-plus Kaiser health care workers whose unions are included in that partnership, a team-oriented framework for every-day decision-making on care and staffing issues that puts nurses, clinicians and others in the middle of the process alongside doctors and company executives.
But the apparent deterioration of the partnership goes deeper — right to the heart of the type and quality of care provided to Kaiser’s 12.6 million members. Roughly 9.5 million members are in California alone; more than a million of those are low-income individuals or families, including hundreds of thousands of children who depend upon timely access to quality care.
For nearly a quarter century after the Labor-Management Partnership was created in 1997, it was hailed by Kaiser as a success and repeatedly cited in labor circles as a difference-maker. The shared decision-making approach, which Kaiser says is the largest of its kind in the U.S., has marked Kaiser as a favored place to work and a desired place to receive care.
Now, that collaborative model is sagging, with members of some unions saying that Kaiser virtually ignores the partnership process when it conflicts with the organization’s larger goals, such as controlling staffing numbers or using technology to perform patient evaluations normally done by trained health workers.
“They’ve lost their direction,” said Kim Mullen, a registered nurse who has worked for Kaiser for nearly 18 years. “There is a true north that they’re off from. I believe they can get back there, but they’re going to need our help.”
Interviews with members of multiple unions over the past few years have revealed similar sentiments. To many longtime Kaiser workers, the cooperative approach of the past two decades is being overridden by a drive for the organization to get bigger, increase its net revenue and swallow up smaller health companies.
In recent negotiations, Kaiser officials have often maintained that such claims were made instrumentally, as a means to win ever-higher wages for workers. In reply to a series of questions for this story, a Kaiser spokesperson told Capital & Main that union actions during some recent contentious contract negotiations “have strained the Labor-Management Partnership and contributed directly to the challenges it now faces.”
The relationship is increasingly toxic. More to the point, the past few years for Kaiser have been marked by a series of grinding, drawn-out labor negotiations and strikes — precisely what the partnership was designed to minimize.
* * *
The labor-management partnership was born of desperation. By the mid-1990s, Kaiser Permanente was losing money at a rapid rate, facing the possibility of companywide labor disruptions, and considering a significant cutback to its operations.
The idea of the partnership grew out of conversations between unions that represented Kaiser workers. Concerned that the cutbacks would wipe out jobs, the Coalition of Kaiser Permanente Unions in 1997 approached management with an idea: collaborate on workplace decisions. The proposal called for front-line caregivers to join the doctors and Kaiser executives who’d previously decided on their own such concerns as staffing levels, scheduling and time spent with patients.
“Everything we do is supposed to be a partnership,” said Zach Pritchett, an emergency room nurse at Kaiser’s Los Angeles Medical Center. “We have things like affordability projects, working together on unit-based teams — all done in partnership.”
In early years, the Labor-Management Partnership was credited with multiple successes, including the rapid planning and development of a new hospital in the Baldwin Park area of Los Angeles County when Kaiser services were critically needed there. Collaborative problem-solving in Northern California improved the organization’s ability to ensure that employees got the breaks and meals they needed while on the job. The LMP was lauded at Kaiser’s Irvine Medical Center for agreeing on ways to reduce the turnaround time on certain surgeries, saving money in the process.
Through this framework, Kaiser also conducted a lot of its broad contract negotiating at a national level, leaving specific details to be hashed out locally. The model’s approach to bargaining is called “interest-based” because it’s built on the premise that a problem for either side at the table will eventually become a problem for the other, so mutual solutions are preferred — a very different model than traditional bargaining, in which both sides present contract offers or demands and then battle until one side or other relents.
Both the Coalition of Kaiser Permanente Unions and the Alliance of Health Care Unions, which collectively represent more than 150,000 workers, are part of the Labor-Management Partnership. About 80% of Kaiser’s union-represented workers are covered by the agreements.
The model thrived for years. Kaiser enjoyed more than two decades of relative labor peace, its partnership-covered union members generally earned more than the local market rate for their jobs, and the organization’s reputation for quality care was enhanced.
Kaiser also regained its financial footing and began to grow. It has added more than 4 million members over the past 20 years and now operates in eight states, plus the District of Columbia. Last year, Kaiser reported holding $67 billion in unrestricted reserves, money that can be used for almost any purpose the organization deems important.
That growth, some union members believe, is fueling the current problems. They see Kaiser as more fixated on increasing net revenue than on adequately staffing its clinics and hospitals. (Because Kaiser’s hospitals and the Kaiser Foundation Health Plan operate on a nonprofit basis, the organization uses the term net revenue rather than profit to describe its income. Its Permanente Medical Groups are for-profit businesses whose doctors are paid by the foundation.)
Examples of its unwillingness to spend in order to improve care, critics say, are Kaiser’s repeated fines, sanctions and labor strife due to its chronically inadequate mental health services. The organization has now paid nearly a quarter-million dollars to state and federal agencies for deficiencies in that area alone — expensive, but less costly than investing in more staff and infrastructure, experts say.
“I don’t believe any other California [health] insurance company has been so heavily penalized in recent years,” said Fred Seavey, research director for the National Union of Healthcare Workers, which represents 2,400 mental health professionals in Northern California. (Disclosure: The NUHW is a financial supporter of Capital & Main.)
“Unfortunately,” Seavey added, “rather than working constructively with its therapists to solve these problems, Kaiser is lowering the standard of care by assigning care duties to unlicensed staff and A.I. bots.”
* * *
Kaiser officials say the organization is not abandoning the Labor-Management Partnership, and they blame union members for making negotiations more contentious than they should be.
“The LMP has helped structure how we engage on workplace, operational and patient care issues, with much of that work occurring at the front lines through unit-based teams,” the organization said in an emailed statement. It added that while the partnership remains an important framework, “It must be grounded in mutual trust, shared responsibility and a commitment to constructive engagement.”
Adrienne Eaton, a Rutgers University labor professor and co-author of a 2009 book that examined the LMP at Kaiser, said she was cautiously optimistic about the future of the partnership. Eaton referenced the “yo-yo model of labor-management cooperation,” with the ups and downs that the term implies.
“I don’t think it’s surprising that there’s been erosion of the LMP during this time,” Eaton said. “But I also don’t think this means the partnership is dead, given the enormous benefits it has had for both labor and management.”
Without question, the past few years have sorely tested Kaiser’s partnership model. The organization narrowly averted a huge nurses’ strike in 2021, and more than 31,000 workers in California and Hawaii participated in a monthlong strike this year that ended in late February after Kaiser and the United Nurses Association of California/Union of Health Care Professionals agreed to the framework of a new contract following months of negotiations. (Disclosure: UNAC/UHCP is a financial supporter of Capital & Main.)
In the runup to the strike, Kaiser officials publicly accused UNAC/UHCP members of trying to degrade the company by threatening to release damaging information about the organization.
What UNAC/UHCP actually released, a report entitled Profits Over Patients, reinforced what a number of unions have asserted in recent years: Kaiser is sitting on a huge surplus but using it mostly to acquire other health systems and invest in other businesses, including the two largest for-profit prison corporations in the country. Kaiser could instead use some of its surplus to improve critical staffing shortages and safety issues within the system it currently runs, the report contended.
Mental health therapists in California have staged multiple strikes since 2022. And the National Union of Healthcare Workers — backed by thousands of nurses — held a one-day strike on Wednesday after filing an Unfair Labor Practice charge in protest of Kaiser’s increasing use of A.I. to perform critical patient tasks, such as asking intake questions that help determine whether or how quickly to schedule care. The NUHW has been without a contract in Northern California for six months.
In each case, union workers said they pressed their demands for increased staffing and schedules that would adequately cover patients’ needs and enable them to do their work properly. In each case, they said, Kaiser pushed back, asserting that at heart the negotiations were really about hourly wages.
Mullen, who has now been through multiple such negotiations as part of the UNAC/UHCP, traces Kaiser’s shift away from the Labor-Management Partnership to the passing of former Kaiser CEO Bernard Tyson, who died at age 60 in 2019.
“Bernard Tyson was the father of our partnership,” Mullen said. “He really believed in it, spoke about it and encouraged the people underneath him to do it — to make sure that we were the best place to work and the best place to receive care.”
Even before Tyson died, though, there were signs of fraying in the Labor-Management Partnership, most notably a statewide strike by mental health care workers in 2019. While Kaiser continues to grow revenue, with the value of its cash reserves increasing from $40 billion to $67 billion in just four years, the organization has spent the past few years almost constantly mired in difficult labor negotiations with the very worker groups it once embraced in the Labor-Management Partnership.
“We remain committed to engaging with our union partners in good faith, while also being realistic about the need for better alignment to ensure the LMP remains constructive, effective, and sustainable,” Kaiser’s emailed statement said. Right now, the idea of the partnership being constructive and effective is at best debatable. Its ultimate sustainability, more than 25 years after its inception, is openly in question.
Copyright 2026 Capital & Main



-

 Imperial DivideJune 3, 2026
Imperial DivideJune 3, 2026California’s Lithium Valley Dreams Meet Reality at the Only Restaurant in Town
-

 Latest NewsJune 1, 2026
Latest NewsJune 1, 2026Deep Cuts to Civilian Support Staff for Families of Deployed Marines Raise Concerns
-

 Column - State of InequalityJune 4, 2026
Column - State of InequalityJune 4, 2026California’s Economy Runs on Labor Trump Wants to Deport
-

 Featured VideoJune 5, 2026
Featured VideoJune 5, 2026At This New Mexico Park, Mountain Bikers Pedal Amid Hundreds of Oil Wells
-

 Latest NewsJune 9, 2026
Latest NewsJune 9, 2026Ousted by the Trump Administration, U.S. Immigrants Remain Locked up in African Kingdom
-

 The SlickJune 10, 2026
The SlickJune 10, 2026Data Centers Are on the Ballot — This Pennsylvania Candidate Won Her Primary Keeping Them Top of Mind
-

 Latest NewsJune 8, 2026
Latest NewsJune 8, 2026The Glacier May Be Gone, but the Love Isn’t
-

 Latest NewsJune 12, 2026
Latest NewsJune 12, 2026California Town Lets Private ICE Detention Centers Police Themselves